

The vertebral bodies encase the spinal cord to provide protection. When stacked on top of each other, they form the spinal column which provides stability for the head and upper body. The spinal cord and the nerve exits are located within the spinal canal.
The intervertebral discs are located between the vertebral bodies. These dics cushion shock forces, acting as “shock absorbers”. The discs in conjunction with the vertebral joints facilitate motion by turning, stretching and bending of the neck.
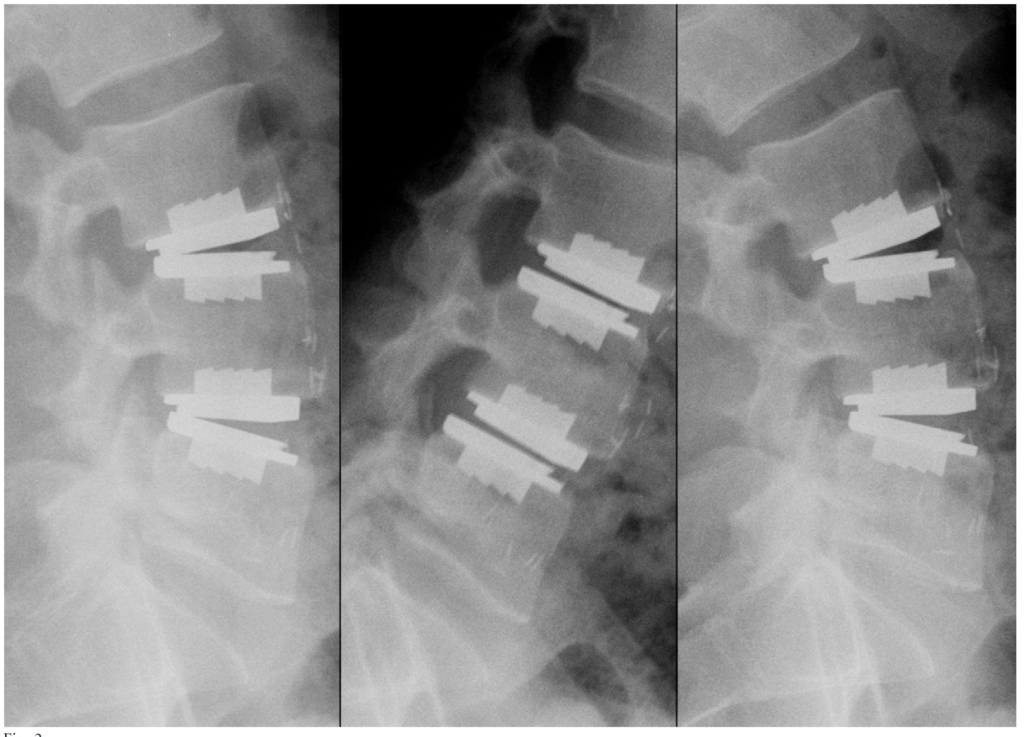
Maintaining Spinal Balance & Motion
Degenerative disc disease can be a segmental destabilizing process. In addition, conducting the surgical procedure to perform a discectomy is inherently destabilizing, since it involves the removal of the ALL, the disc, and often the PLL. In the absence of these restricting structures, it is important that a disc replacement have constraints, in order to protect the facet joints.
In order to provide constraint, the prodisc mechanism of action enables movement with a fixed center of motion, enabling A/P translation only with flexion / extension.
Decelerate Adjacent Level Reoperations
The ‘gold standard’ for treating degenerative disc disease is to conduct a fusion and fuse the joint. However, immobilizing a segment of the spine has been shown to increase the rate of adjacent level degeneration. By enabling motion, prodisc is intended to decelerate adjacent level degeneration. A paper published on the results with the US IDE PMA clinical study showed that, at five years follow-up, patients had 3.5 times more development of adjacent level disease with fusion than with prodisc L.
Accelerate the Resumption of Activities of Daily Living
The operative procedure to conduct a discectomy can be invasive and require recuperation. Special care has been taken to design the technique and instrumentation to minimize the recuperation and recovery associated with the procedure. In a study comparing prodisc L and circumferential fusion, surgeons found that patients that received the fusion treatment option lost nearly twice as much blood during the procedure (794mL vs 410mL), spent nearly twice as much time in the OR (344 minutes vs 185 minutes), and spent longer in the hospital (mean stay of 4.78 vs 4.32 days)[1].
[1] Levin DA, et al., Comparative Charge Analysis of One- and Two-Level Lumbar Total Disc Arthroplasty Versus Circumferential Lumbar Fusion, Spine, Vol. 32, Number 25, pp2905-2909.
Our vision is to provide excellent, patient-focused, comprehensive orthopedic care to patients of all ages across North Georgia. With more than 20 years of experience, Specialty Orthopaedics has grown to become a pillar of the North Georgia medical community with four convenient locations in Gainesville, Dawsonville, Braselton and Duluth.